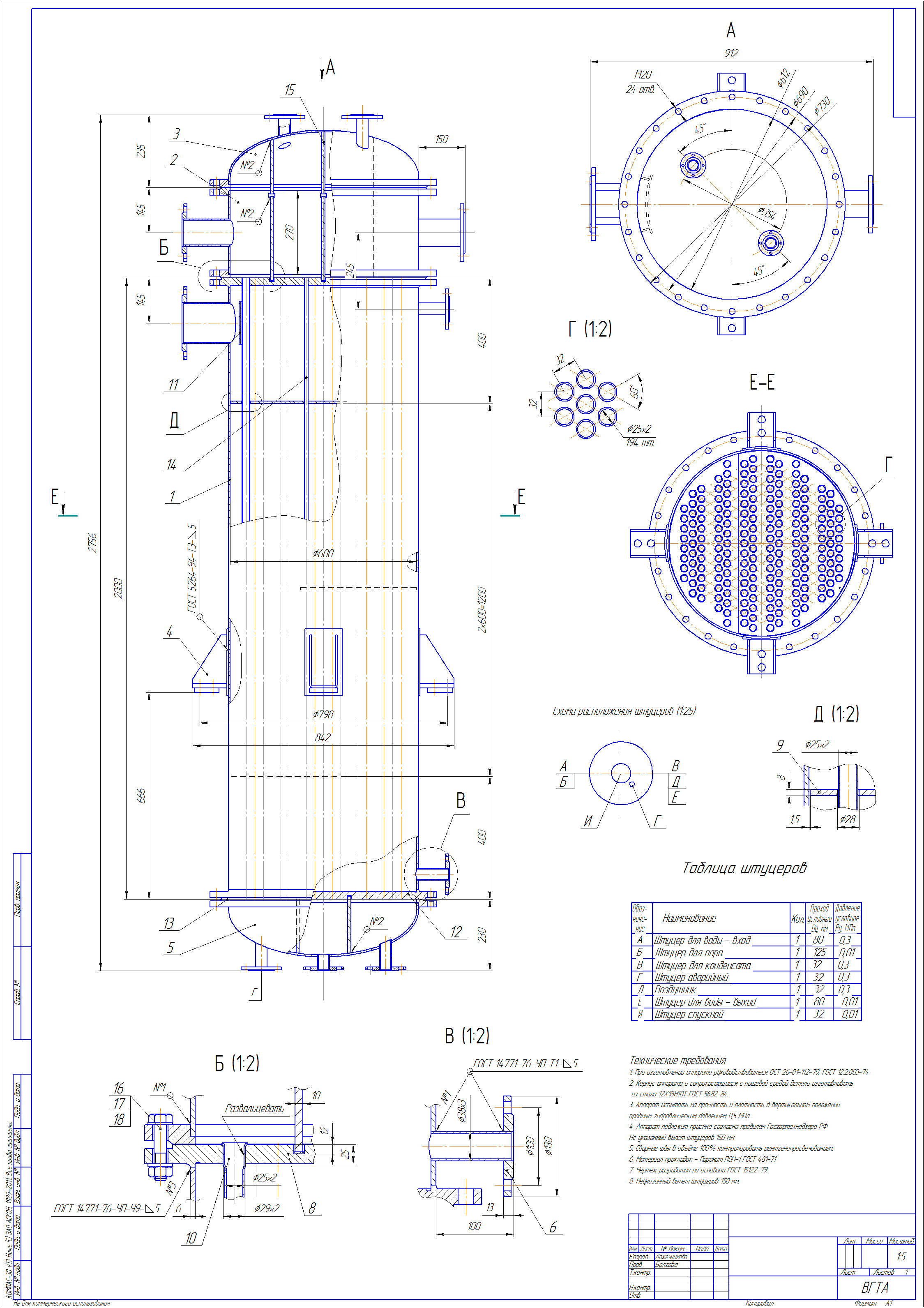
Chertezh Kompas Isparitelj Kozhuhotrubchatij5100944
Search the world's information, including webpages, images, videos and more. Google has many special features to help you find exactly what you're looking for.
Herpes Zoster Ophthalmicus Varicella-zoster virus (VZV) is another neurotrophic virus that has a predilection for the trigeminal ganglion. The primary infection usually occurs in early childhood as chickenpox, which got its name from the blisters on the skin that resemble chickpeas. Primary infection with VZV is nearly universal in childhood but can be so mild that it is missed. However, if acquired in infancy or adulthood or by immunocompromised persons, it can be fatal. Unlike HSV, VZV becomes latent in multiple ganglia simultaneously. It reactivates, usually in the elderly, as a vesicular rash commonly called shingles.
The name derives from the Latin cingulum, which means girdle or belt, because of its distribution along a single dermatome. The exact triggers for reactivation are unknown, but decreased cellular immunity is common in those who have shingles. It is estimated that 95% of adults in the United States have antibodies to VZV and that 300,000 to 500,000 individuals are affected by shingles each year. Of these herpes zoster cases, approximately 25% are herpes zoster ophthalmicus (HZO). Diagnosis The brief prodrome of HZO consists of fever, malaise, and chills.
The initial symptom is hyperesthesia or paresthesia, which may be severe, along the affected dermatome. This is followed by a maculopapular rash that becomes vesicular and finally pustular before crusting ( Figure 9). One common feature of HZO is severe eyelid edema that accompanies the rash and that can be mistaken for preseptal cellulitis. If the tip of the nose is affected by reactivation along the nasociliary nerve (as manifested by the appearance of cutaneous vesicles—the Hutchinson sign), there is almost always ocular involvement. 
Although the Hutchinson sign is a good rule of thumb, it is neither sensitive nor specific, and ocular involvement can occur in the absence of this sign. Ocular zoster can affect any part of the eye from the conjunctiva to the optic nerve. It can cause keratitis, scleritis, uveitis, trabeculitis, choroiditis, acute retinal necrosis, optic neuritis, nerve palsies, and cavernous sinus thrombosis. Discussion of these noncorneal infections is beyond the scope of this module.
Keratitis can be classified as acute or chronic/relapsing, both of which can lead to long-term sequelae. Acute Keratitis Acute keratitis can occur up to 1 month following the onset of dermatitis. Some of the common manifestations include the following. Punctate keratitis and pseudodendrites consist of swollen, poorly adherent epithelial cells and are usually seen in the corneal periphery and appear “stuck on” ( Figure 10). In contrast to HSV dendrites, these pseudodendrites lack terminal bulbs and dichotomous branching and stain poorly with both fluorescein and RB.

Although VZV has been cultured out of these lesions, they do not respond to topical antivirals. Nummular keratitis is characterized by coin-shaped (nummular) lesions that appear in the superficial stroma. The lesions usually underlie areas of previous epithelial keratitis. They probably represent an immune-mediated stromal reaction to viral antigens.
HZO-related keratouveitis and endotheliitis resemble HSV keratouveitis and endotheliitis but are usually more severe, even leading to the development of a hypopyon or hyphema. Involvement of the trabecular meshwork can lead to severe glaucoma that may be unresponsive to glaucoma medications but responds to steroids. Sclerokeratitis occurs as a crescent-shaped corneal infiltrate adjacent to an area of scleritis. It is clinically identical to nonherpetic peripheral ulcerative keratitis, and the etiology is thought to be limbal vasculitis and ischemia.
Chronic/Relapsing Keratitis This form occurs up to several months following the initial HZO infection. Mucous plaques can occur suddenly in an eye that has been nearly quiescent. They appear as stuck-on, grayish, branching lesions and have minimal underlying inflammation ( Figure 11). Mucous plaques stain with RB, and they can be easily wiped off the cornea, leaving an underlying epithelium that is intact but poorly adherent. Cyberlink powerdvd 13 free download full version for windows 7. Therefore, they are thought to be a variant of filamentary keratitis, although some investigators have found viral DNA in the lesions.
Mucous plaques can be highly resistant to treatment, and multiple recurrences can lead to scarring. Disciform keratitis is similar to the disciform keratitis seen in HSK. Interstitial keratopathy: HZO keratitis can lead to vascularization, with a leash of vessels leading up to the area of scarring. These vessels can exude large amounts of lipid that can cause significant corneal opacification. Long-Term Complications As in HSV keratitis, neurotrophic ulcers can occur repeatedly and cause problems long after the acute episode has resolved.